

Life is full of twists and turns, so there are lots of times we need to start over in one way or another. There are eras to life – chapters to open and close. And no matter what chapter has been opening for me, I’ve always brought along one thing – my gardens.
Everywhere I’ve lived, my green thumb has begun throbbing and begging me to recreate the outdoor space I’ve been assigned. I can’t help it. I love landscaping and plants, so it just comes naturally to me. Making art with plants is fun. A garden is a living artwork that changes through the seasons, and it’s easily adjusted if one doesn’t like the results of their first attempt. Or second. Or third. It’s a canvas where one can just play all the time, a canvas where nothing is permanent.
Even at my first big city apartment in a concrete jungle I found a way to sneak in some annual flowers around our tiny cement patio to brighten things up a bit. Our first little house in Del City, Oklahoma was just a tiny thing sitting on a little square of Zoysia grass with literally no plants, trees, or shrubs around the place. By the time we left it had a beautiful hedge, front garden, and a massive vegetable garden out back. Our second place in Des Moines. Iowa was a small fairytale-like cottage with unmanaged trees and shrubs and too much backyard cement. By the time we left, there were annual and perennial gardens all around the house, a vegetable garden, a terraced garden off the driveway, a water garden, and a finch aviary beside the garage. Our next place, in Grinnell, was way out in the countryside. Twenty-seven acres of old oaks, second growth woods, hills, ponds, and pastures. Here I removed all the fencing, built another pond, managed the woods, converted the pastures to native prairie grasses and forbs, did prairie burns, built a new house and donated the old house; and created terraced gardens, water gardens, and vegetable gardens. Specimen trees and native trees were added here and there. It was a sanctuary for us and for wildlife and plants. I could have spent a lifetime there – it was my ideal place.
My next place was in town. A historic 108-year-old craftsman style stucco house on a tiny corner lot. Here I made a new type of garden, a fenced English-style back garden blending a combination of formal plantings and native woodland plants. Once again I had a water garden, this time with tropical fish. The barren front lawn became a gorgeous array of trees, shrubs, and native and ornamental perennials. And I tried something completely new – a moss garden. The space was small but had lots of microenvironments and therefore needed micro gardens to fit them. By the time I left, the outdoor space there was a wonderful hidden refuge that looked like it belonged in a tropical rainforest.
And now I find myself in Connecticut, a place that is a far cry from both Oklahoma and Iowa as far as gardening goes. I was surprised at how wooded this state is; in the past the entire state except for the northwest corner had been cleared of trees and converted to little farms. Today it is densely populated and semi-mountainous, with scattered farms the farther east you go, and orchards and vineyards the farther west. The woods are thick, and the homes are often spaced widely apart, so in the spring, summer, and fall, one doesn’t even notice most of the houses. It just seems like you’re driving through the woods. It’s a spectacular landscape. The roads are all winding – nothing here is on a grid. The rivers are clear. There are burbling stone lined brooks and streams everywhere one turns – gorgeous water the likes of which I never saw in Iowa or Oklahoma. And because of the nearby Atlantic, the temperatures and general conditions are temperate and less variable than anywhere else I’ve lived. Intense cold doesn’t last long, and neither does intense heat. I get all the seasons with less weather drama. I do miss the intense thunderstorms of the Midwest, though. Talk about weather drama! The thrill of those powerful winds sweeping over the open land, the lightning, the thunder, the downpours, the gigantic hail, the constant threat of a tornado or blizzard wrecking everything – I loved it. Connecticut is nothing like Iowa or Oklahoma. It’s calm and neutral in comparison. I’m actually in zone 6 for plant hardiness now! I can grow things here that I could never succeed with in Iowa in spite of my green thumb. There is no winter deep freeze out here like the Midwest has, and no blasting of hot air for days on end at the height of summer. It’s humid, but not like the humidity of summer corn sweat in Iowa. The weather out here seems like a piece of cake in comparison.
The place we finally found after two years of searching during the worst housing market on the planet is a smallish house on one acre at the bottom of a mountain on the east side of a state park. It was a lucky find even though it cost twice as much as it should have in my opinion. It was badly overgrown. The house had a million things wrong with it, as did the outside gardens, driveway, and patios. The house sort of sits on a little cliff overlooking a small pond fed by a mountain brook and drained by a little spillway. The road is quiet, as the street is really just a long cul-de-sac that goes halfway up the mountain, so there’s almost no traffic. Across the road is a classic New England gentlemen’s farm with a house built in the 1800’s, a cool old barn, and a couple of horses on a little pasture, just enough of an open space to give my Midwestern eyes some relief from the dense woods all around. Our house was built in 1960. The owners planted white pines all around, some of which are well over a hundred feet tall. I guess they do well out here. They’re kind of terrifying, really. I keep wondering when they are going to fall on the house and kill me. But when storms come through our area, the woods all around and the mountain behind shelter the massive white pines from the brunt of the wind, and although they move around a lot, they seem to be perfectly stubborn in their grip to the earth. I don’t think they’re going anywhere, possibly for a hundred years. Who knows?
Our place is surrounded by second growth woods owned by the man across the road. Across the pond to the east is a large stand of black walnuts. To the south is mixed woods, and to the west is mostly sugar maples. The woods have not been managed, and Connecticut has a serious problem with invasive plant species, so our little property was being severely encroached upon by honeysuckle, bittersweet vines, Japanese Knotweed, multiflora rose, Bartlett pear trees, and burning bushes – all of which are affecting the growth of the large forest trees. In the south woods nearly every large tree was dying due to strangulation from bittersweet, Boston Ivy, grapevines, and climbing poison ivy. I asked the landowner if I could start doing some things in the woods to help the trees and he said fine as long as I don’t take down any healthy trees. Well, there was no danger of finding a healthy tree in that part, let alone taking one down! The invasive shrubs needed to be cut down and all of the vines shrouding the trees needed to be cut off at the base. That one simple maneuver would once again let the sun in so the trees and native forest floor plants could recover and thrive.
The brook flowing into the pond was overgrown as well, mostly with multiflora rosebushes. I hate that plant. It was all over Iowa too. It was brought in from Asia years ago to form livestock hedges, and it works. It’s a vicious plant with recurving thorns that grab you and won’t let go. It has to be chopped out with the base poisoned or monitored for new growth. Its only natural predators are a virus that kills it sometimes, and goats, which you have to tie to the shrub. I don’t know how they can eat it without bleeding to death, but they do. The seeds are spread by birds, and it just comes up everywhere. It can be killed by cutting it back repeatedly month after month, which though time consuming, is better than putting herbicide in the environment.
The far side of the pond had ALL of the invasives. They were growing so aggressively they were climbing right into the pond. Where was the edge? It turns out it was, in some places, twenty feet back from where the plants were invading the water. And then there was some horrible invasive grass growing around the pond that I have been unable to identify; it has tiny silica barbs all over the leaves and stems which will cut you to ribbons if you try to remove it without gloves and a long-sleeved shirt. And then there was the poison ivy, my god. It had completely covered the edges of the yard, the slope in front of the house, and a huge swath along the driveway. It had literally buried all sorts of artifacts placed by previous property owners, like a little arroyo down by the pond, boulders, and a cement Chinese dragon dog statue. It turned out that about 100 square feet of the lower patio was covered with a layer of dirt and grass a foot deep. I just kept finding things, hints of what had gone on there in the past sixty-five years. I started feeling like an archeologist.
In front of the house and along the drive there had once been well-manicured formal gardens. They were still there, still pretty, but unkempt. Many plants were not in the correct place considering the available sunlight. Some were struggling. But clearly someone in the past had known their ornamental plants and knew something about garden design. There were many fine specimens buried in there that had to be uncovered, and later, many that had to be moved to more suitable environs.
It took a year and a half to get it all cleaned up. The pond is now an oasis with flowering water plants along the edges and floating lily pads in the middle. A little dinghy with wooden oars is roped to the bank. The brook has been uncovered and made into a series of little waterfalls. In the spring it is infiltrated with skunk cabbage, a plant that melts the snow with it stinky huge flower in late winter, then later puts out giant leaves that look like hostas. I planted a miniature conifer garden, an herb garden, and a vegetable garden by the lower brick patio. Two hundred tulip and daffodil bulbs went in all around the house this fall. The soil has been a challenge, with all of its rocks and variable nutrient values; it was hard to plant bulbs. A Zen garden has been added behind the house. Flowering and ornamental trees have been added, along with many shrubs. The forest all around has been cleared of many invasive plants and unnecessary saplings. The grassy areas all around the pond have been overseeded with native wildflowers for bees, butterflies, and other insects; these areas will no longer be mowed as they were in the past, and within two years it will change the surrounding ecosystems. Last year there was a pair of Mallards looking to nest somewhere beside the pond, but there was no place for them. The far side was too overgrown, and the rest was too exposed due to mowing. Next year they will be able to find a place. I put up two wood duck nest boxes, so maybe we’ll have those too. This summer three river otters showed up in the pond! There are Canada geese across the road on the pasture, and there’s a kingfisher and a blue heron that spend a lot of time catching bullfrogs out there. There are blue crayfish and little salamanders in the pond, and other types of frogs and toads in the tall grass. I’d like to make a fish ladder by the spillway to see if any trout might migrate to the pond and on upstream in the spring to spawn.
We have been startled by the wildlife out here. Lots of songbirds. Lots of black bears. Bobcats. Hawks. Grey squirrels. Deer. Chipmunks. Snakes. Coyotes. Foxes. Apparently even fisher cats have re-entered the state. Where are the mountain lions, I wonder. Frankly, it’s perhaps a little dangerous. We don’t walk around outside here after dark. I have to warn the granddaughters to check for bears, bobcats, and coyotes when they walk out the door and to be aware of their environment at all times. We have to teach about deadly ticks, poison plants, and mosquitoes too. Living in the woods is not for the faint-hearted. You have to learn a lot and pay attention to what’s going on around you.
And the drivers! If you don’t get killed in the woods, you certainly may on the road! I’ve never been any place where people drive so badly! Tailgating, no turning signals, speeding and swerving in and out of traffic, and running red lights are the name of the game. Everyone is in a rush except for me. Thankfully our little town is pretty quiet, but every time we leave our little forest oasis, we have to drive like A.J. Foyt. The Mini Cooper goes into sports mode and off we zoom! If you can’t beat ‘em, join ‘em.

“We are way past the point when health care should have been overhauled in the U.S. No one should have to be worried about being bankrupted by the insurance companies or denied care. No one should have health insurance that is tied to employment. No doctor should have to put up with abuse and manipulation from the insurance companies. Health care should be available to all whenever it is needed, period. It should be broadly government supported. And all private health insurers should be not-for-profit. Medicare should have been made the national health care insurance program for everyone when it very first began, starting with birth.” – David Coster, Coz Blog (cozmd.com), “A Slave with Two Masters.”
Yes, I’m quoting myself. I wrote the above when United Health Care was finally publicly raked over the coals for ruining the lives of the patients who were paying them for health care coverage by refusing to pay for necessary medical care. The problem yet continues, unabated, in spite of public outcry, because our politicians enjoy getting bribes from health industry lobbyists.
And now, the Trump administration has made matters even worse with their plan to stop subsidizing the Affordable Care Act, an Act that was put into law with great effort and a bipartisan vote on behalf of all Americans during the Obama administration in 2010. The Republicans argue now, today, that the government is being taken advantage of by the insurance companies to whom they pay the subsidies on behalf of poor and middle-class Americans, so the program should be scrapped. I couldn’t agree more that insurance companies are taking advantage of government taxpayer money. The proposed solution? Send the money directly to the citizens instead, though there is no such legislation in process and no details of how such a plan might work for the average American. No one has mentioned the idea of reigning in the health insurance companies which had record breaking profits this past year, profits they earned by refusing to pay for necessary health care while overbilling the government for the ACA patient subsidies, both problems that could easily be solved by Federal legislation if the Republicans cared to make it happen. Republicans refuse to extend the Affordable Care Act while this gets sorted out, an obvious potential temporary solution. No one mentions the obvious solution of universal health care
Meanwhile, with the threat of this change hanging over the heads of our wonderful capitalistic health insurers, they have jacked up health insurance premiums for 2026 across the board and, in some cases, by as much as 300%. In some cases, the cost is so astronomical it will take the majority of an individuals annual income to pay the premium, not counting the out-of-pocket expenses that amount to thousands of additional dollars.
How are people doing to deal with this? I’m going to go out on a limb and say that more than half the population of the United States cannot just conjure up an additional tens of thousands of dollars per year for health insurance premiums at a moment’s notice, if at all.
This is what will happen. I can tell you how it will go. When it becomes clear to the public that no insurance company on the insurance exchange will be providing subsidized health insurance anymore and the premiums have increased to $15,000-24,000 a year or more (plus copays and deductibles), most Americans will simply go bare. No health insurance. And without health insurance, they will not even go to a walk-in urgent care clinic due to the cost, even when they are sick and should go. They will stay home until they become incredibly sick. Only then will they seek care. And when the ambulance company determines they have no health insurance, they either won’t go to pick them up, or if they do, they will charge tens of thousands of dollars for the ambulance ride. Once the patient arrives at the ER in an ambulance or the family car, by law they have to be seen, at least as of today. I imagine the Republicans will get rid of this rule as well as soon as they can. But for now, the ER cannot turn them away, so the ERs around the country will be inundated with very, very sick patients, patients who couldn’t buy insurance and so didn’t get their medications or other treatments they needed that could have kept them out of the emergency room. The ER docs will see them and admit them to the hospital because they are morally and legally required to do so. And because they are very ill, they will spend several days there being treated. And since they have no insurance, the hospital will bill them at the top rate for their care – the absolute maximum they can get away with. The patient will recover and go home, still without insurance, still without money for medications, still without the necessary medical support they need, and the whole scenario will repeat itself. Within days of their discharge, they will be getting letters from the ambulance, doctors, and hospitals indicating they owe hundreds of thousands of dollars. They will be unable to pay, so the hospital will put a lien on their property, a lien on what little they have in their bank account and then attempt to take it all. If the patient can find a bankruptcy attorney, they will file for bankruptcy, an act that will have economic consequences for years. The patient may subsequently die or become homeless. That’s how it will go all over America, so get ready for it.
In addition, of course, many hospitals required to care for all of these uninsured people will go bankrupt, as will physician offices, nursing homes, surgery centers, and so on. You can’t squeeze blood out of a turnip – people who have no money for insurance also have no money for big hospital bills, so no matter how hard the private health system works to collect the money it is owed from the poor and middle class, it will be able to retrieve only a fraction of what it lost through collections and legal maneuvers. Rural hospitals will close everywhere. Many urban hospitals will close. People will simply die due to a lack of access to any medical care. Those working in the field, such as doctors and nurses, will simply give up and walk away due to financial and moral exhaustion. We will go back to medieval medicine. Herbs and leeches. We’ll live 35 years on average if we’re lucky. This is the future of health care in America today.
And yet there is even more that can be done to make it worse: “Let’s see, we know there is a drastic shortage of physicians, nurses, physical therapists, physician assistants, nurse practitioners, and so forth already, but we think it’s in the best interest of all Americans to pretend that education for these professional careers does not count as professional education, so we are going to limit the amount that any person can borrow for student loans to get the necessary education for those careers.” You can thank Linda McMahon, Donald Trump, Mike Johnson, Robert Kennedy, and the other nitwits and criminals left in charge of the operations of the United States government for this brilliant maneuver. And you can be sure that whenever the shortage of health care professionals hits crisis level, which it is approaching, congress and the president will make sure they get the best medical care possible while Americans everywhere else die left and right.
No one in their right mind would choose to go into any sort of medical career in America in this scenario. Millions and millions of patients will overwhelm what few providers we have. They will, of course, burn out and quit, regardless of how altruistic they might be.
This is where we are, America. This is what our leaders have done to us. We had a chance a couple of decades ago, a fighting chance, to put all Americans on Medicare, a universal health insurance program that is NOT FOR PROFIT, a program that applies 98% of its revenues directly to health care and only 2% of its revenue to administrative costs. The for-profit insurers spend only 64% on direct patient care; the rest goes to administrative costs which include massive multi-million-dollar salaries for the CEO and other higher-ups, and dividends to stockholders. Because it’s not for profit, Medicare premiums cost 75% less than private for-profit insurance, and the poor pay next to nothing. But when the idea of Medicare-for-All was floated back in the 2000’s, the FOR-PROFIT insurance companies such as United, Aetna, Blue Cross, Anthem, Kaiser, and others lobbied against Medicare-for-All with all their might and stopped it dead in its tracks. The Affordable Care Act was a bipartisan (both the Republicans and the Democrats) agreement that was the compromise for not switching to Medicare-for-All. It wasn’t good enough, and everyone knew it, but it was better than what we had before and gave access to health insurance for millions of Americans, insurance they otherwise could not afford. It was as good as could be gotten with a congress that was/is in the pocket of the for-profit health insurance companies, and those of us in the medical field noticed the effect immediately. No longer did we see patients without insurance. No longer did I have to convince the hospital CEO to let me do surgery for poor patients for free. No longer did our rural hospital have to struggle constantly for adequate payments to keep it in the black. No longer did we have to run short-staffed. Literally everything got better for our patients and our hospitals after the passage of the Affordable Care Act.
I’m of the opinion that our ridiculous American experiment of health care coverage tied to employment is over. The United States is the ONLY country that does health insurance this way. The handwriting is on the wall, and no doubt the private sector knows it. This stupid experiment didn’t work. So, what are they to do to keep their investors happy and keep rolling in the dough? How about going on a rampage to rape and pillage what few people/families remain who can pay these new outrageous premiums, beginning January 1st, 2026? Of course! They have to line the pockets of their CEO’s, stockholders, and upper management with as much money as they can before government money gets shut off because regular Americans are PISSED OFF. This for-profit insurance company gravy train needs to go off the rails. Every other civilized nation has access to tax-based health care with minimal or no cost associated with visits to clinics and hospitals. The action by Republicans in passing the Big Beautiful Bill, ending the only insurance program that was helping the poor and middle class – the Affordable Care Act – may, ironically, prove to be the end of the current health care system in the United States and likely force the changeover to universal health care. I imagine this is not what the Republicans anticipated considering their rabid support of pure capitalism, but there it is. They will have inadvertently done some good if that happens. The problem is they laid no safety net for the millions who will lose their insurance in the meantime.
There is a simple solution, and pure capitalists won’t like it in concept but will in practice, because people in every other civilized democratic society, all of which have combined socialist/capitalist democracies – do. The government – if it’s ever stable again – should take control of the health care system and roll all private health insurance companies into Medicare and switch the entire system over to Medicare rules. No more public investors, no more massive salaries, no more wars between health insurance companies for market share, just one electronic medical record instead of dozens that can’t talk to each other, no more battles between doctors and insurance companies, no more pre-authorizations, no more BULLSHIT.
“You socialist!” some might scream at me for even suggesting such a thing. And to that, I have to ask: Who’s in charge here, the three hundred and fifty million people in this country, or a couple dozen CEO’s who are raping the American public to the tune of trillions of dollars every year and leaving millions of Americans in the poorhouse and/or without health care? NO OTHER “FIRST WORLD” COUNTRY HAS ALLOWED THIS TO HAPPEN TO THEIR PEOPLE! Over seventy countries have universal health care that doesn’t break the bank for their citizens!
But what about the upper middle class and wealthy investors?! They’ll lose their mutual fund and stock profits from their health insurance company and for-profit hospital investments! Yes, they will. But they’ll get guaranteed tax-supported health care at no additional cost and if they value it as much as they do the value of their health insurance company stocks it will be worth the trade. Consider it an investment in a better society and shut up.
If you really want to make America into something great, it’s going to require the full application of the concept of a socialist-capitalistic democracy, a place where socialism applies to the aspects of life and the economy which require all of us to cooperate and help each other, such as health care, transportation, safety standards, food supplies, energy, scientific research, education, and housing; where capitalism applies to entrepreneurship and types of businesses that do not affect the survival and safety of the people; and where democracy applies to the right of the citizens, not the politicians, to dictate how it will all go.
The term abortion means the early loss of a pregnancy. This can happen in various ways. By far the most common way is what is called a spontaneous abortion, or miscarriage. Spontaneous abortions occur frequently, in up to 30-40% of pregnancies, and typically between a few days and 12 weeks after the blastula/blastocyst implants into the lining of the uterus. (A fertilized egg turns into a blastula, a ball of cells that has the potential to develop into an embryo.) Thus, nearly a third of all women attempting pregnancy will suffer a spontaneous abortion during their reproductive years, and some will suffer several. Such spontaneous abortions, or miscarriages, are not the fault of the mother. The reasons they occur are many, including genetic abnormalities, hormonal imbalances, immunological abnormalities, and improper development of the early embryo. In most cases such abnormalities will result in the uterus expelling the failed pregnancy spontaneously in a bloody mess called a miscarriage. If all goes well, it is all expelled quickly, and the uterus clamps down and stops the bleeding. If things don’t go well, the miscarriage may only partially come out. This is called a failed partial miscarriage. In that situation the uterus cannot clamp down and stop the bleeding, so the woman may bleed to death. Sometimes the early embryo will simply die or be absorbed but there is no progression to discharge of the placental tissue and amniotic material; an ultrasound will show a tiny amniotic sac remaining in the uterus with nothing in it, or a tiny dead embryo. This is called a failed miscarriage. The presence of the material will prevent any new desired pregnancy from occurring. Some sort of intervention has to occur so the woman can try again.
In the past, the only way to treat a partial spontaneous abortion or missed spontaneous abortion (partial is dangerous due to retained tissue with bleeding and risk of infection; missed abortions can be monitored for a while, but problems such as bleeding and infection can occur later if one waits too long for treatment) was to perform a dilation and curettage, a D&C. This is a minor procedure. The woman is given a general anesthetic. After sterile preparation, the cervix of the uterus is grasped with an instrument and the opening in the cervix is probed with gradually enlarging dilators until the opening has been dilated to about a half inch. Then, a blunt curette – a smooth instrument with a little metal loop on the end – is inserted and gently swished around the inside of the uterus and retracted, pulling the miscarriage material out. The curette is passed a few times to be sure everything has been removed. The uterus is examined to make sure it has contracted down, and the cervix is observed to make sure there is no active bleeding. The specimen, consisting of a tiny placenta, remnants of the embryo (if it exists), the amniotic membrane, and the lining of the uterus (endometrium), is sent to the pathologist for analysis. Sometimes it can be determined why the miscarriage occurred based on study of the specimen, including DNA analysis. Most of the time, the cause remains unknown.
The treatment for a spontaneous abortion (miscarriage) should never be politically or religiously controversial. There is no living embryo in any such case, and treatment is required to protect the mother from bleeding to death or dying from infection. Treatment also preserves fertility so the woman can try again for a successful pregnancy. I have performed this procedure many times for women with partial or missed spontaneous abortions (miscarriages). It is routine surgical care.
More recently, hormones and medications have been used to help the uterus expel entrapped material from a partial or missed spontaneous abortion (miscarriage). The medications cause the lining of the uterus to detach (like a period) and stimulate the uterus to contract to push out the lining and the material left from the failed pregnancy. This is routine medical care that can be chosen as long as the patient is stable and meets necessary criteria. Again, in all of these cases there is NOT a living embryo in the uterus. It has already perished. This is why treatment is needed.
I want to be clear that in the case of any type of spontaneous abortion (miscarriage), the pregnancy has failed of its own accord. There is no life in the uterus – no blastula, no embryo, no fetus. The purpose of all treatments is to bring the mother back to good health and maintain fertility.
What’s an “”ectopic pregnancy?” An ectopic pregnancy is a pregnancy located outside of the uterus. The fertilized egg somehow manages to implant and begin to grow where it is not supposed to. Typically, such pregnancies are located somewhere in or on the “adnexa.” The adnexa is a term referring to the ovary, the fallopian tube, and the various ligaments that support those structures and the uterus in the pelvis. So, the blastula implants on an ovary, on a ligament, or on or in the fallopian tube. In even stranger cases, the blastula may implant within a c-section scar, on the intestine, in the liver, or on some other organ. By the time symptoms appear at a few weeks after implantation, there is a tiny embryo with an attached placenta that is invading the structure supporting the pregnancy. Often the very first symptom is sudden pain followed by severe bleeding within the abdomen, as the pregnancy has ruptured. This is an emergency. There is no such thing as an ectopic pregnancy that is viable if it has ruptured, i.e., none can survive. In other words, no such pregnancy can ever produce a baby – all it can do is kill the mother. Immediate surgery is the treatment if the patient is bleeding and unstable. If the patient is symptomatic or asymptomatic but not bleeding, a cancer treatment drug might be used to destroy the embryo and placenta, but usually surgery is necessary. Often an ovary or tube or both will need to be removed. I treated many ectopic pregnancies in my career as a surgeon. It is typically impossible to identify any embryo in the material removed; it is too small and degraded to even be visible. Every once in a blue moon a fetus manages to develop in an ectopic site and get to the age of viability – 23 weeks gestation. Such occurrences are incredibly rare. The situation is touch and go and has to be carefully managed by experts to try to save both the fetus and the mother. Surgical intervention is invariably required if an ectopic pregnancy gets that far.
Treating an ectopic pregnancy is like treating a miscarriage, but more complicated. It’s always either an emergency or an urgent situation. Some people seem to be confused about that. To be clear, treatment is not optional, it’s mandatory and medically required in order to save the mother’s life. This should not be politically or religiously controversial, and the subject is too complicated to be relegated to the whims of a legislature or congress.
When deliberate steps are taken to end pregnancy, the term used is induced abortion or early termination of pregnancy. This is done with the full knowledge that there is a living embryo (it is an embryo until ten weeks gestation) or fetus (defined as after ten weeks gestation when it takes on the form of a tiny one-inch human) within the uterus. The reasons for terminating a pregnancy, or having an induced abortion, are many. Two reasons are severe developmental abnormalities not consistent with life outside the uterus, and genetic abnormalities not consistent with life outside of the uterus; it is justifiable to recommend a medically induced abortion or surgical abortion (usually D&C) in such cases to reduce the risk of complications of pregnancy for the mother and to allow her to make another attempt at a successful pregnancy as soon as possible. It is hard for anyone to validly argue against abortions in such cases. Carrying a pregnancy just to watch a fetus or infant die in the mother’s arms is not more humane than an early termination, and such complicated pregnancies place the mother at additional risk for life-threatening complications.
And then there are more controversial circumstances, such as a pregnancy that is the result of a rape or incest. Often these cases involve minors and there is nothing wrong with the embryo. In many cases the victim is so young that carrying the pregnancy to term may be physically dangerous, not to mention psychologically and emotionally traumatic. If the victim is an adult, they may have a strong psychological and emotional aversion to giving birth to the child of the man who raped them. Either way, the decision to proceed with the pregnancy or not is highly complicated and is not something that can be easily relegated to legislation. Nevertheless, the argument is made that it’s not the fetus’s fault that it was conceived in violence. Some therefore think the mother should be forced to bring it into the world regardless, putting her once again at the (small) risk of death or physical harm and the higher risk of mental health and social consequences. The theory is that if she gives birth, she will bond to the baby and love them anyway or at least be able to give it up for adoption. For those who think the mother should be forced to maintain the pregnancy and deliver the baby, one is left to wonder why they think their viewpoint is relevant – they have no skin in the game. We all have feelings about this conundrum, but I can’t help but think that such feelings should be applied only to one’s own circumstances, not those of others.
And finally, there is the highly politically charged medically induced (almost all) or surgical (far fewer, and usually by D&C) abortions done by “choice.” These abortions are associated with unwanted pregnancies and pregnancies that may be inconvenient or burdensome to the mother/family due to economic, personal, professional, or social hardships. These are the abortions most people are talking about when they say they are “against abortion.” Most such induced abortions today can be performed by D&C but are usually not performed by D&C, as there are less invasive methods available. Rather they are induced by medication very early in pregnancy when there is only a fertilized egg, a blastula, or an embryo. The morning after pill is a special treatment that uses hormones as a precaution to prevent a possibly fertilized egg from implanting in the uterus – it prevents a pregnancy from occurring in the first place so cannot properly be called an abortion. (The vast majority of fertilized eggs in humans naturally don’t implant – they just come out with the monthly period.) Mifepristone and misoprostol are medications used throughout the embryonic phase (up to ten weeks gestation) to induce an abortion. A fetus, defined as 10 weeks and on, cannot live outside the uterus until they’ve reached 23 weeks gestation. The more premature the fetus, the less likely it will survive or survive without complications.
And then there is this other thing, the so-called “late term abortion.” The definition of “late term” is not settled, but it seems to be anything after fourteen weeks, or early mid-trimester. The reasons for performing such a procedure are typically extraordinary and related to the mother’s health, i.e. the mother has complications of pregnancy that are going to kill her if the fetus is not removed urgently. Such conditions could include a new diagnosis of an illness, such as cancer in the mother that must be treated right away with medications that cannot be taken during pregnancy, or conditions such as severe preeclampsia or eclampsia that are caused by the pregnancy and will kill the mother if the fetus is not delivered or removed. Women who develop cancer or another life-threatening illness after the first trimester will typically delay their own treatment until the fetus has reached viability (23 weeks or later) and simply undergo an induction of labor or a c-section to deliver the fetus early so they both have a chance of survival – this is not an abortion. It is delivery of a live fetus early in order to save both the fetus and the mother. Some women choose to sacrifice the fetus to save themselves if the age of viability is too far off for her to survive long enough to possibly save the fetus (they may be too ill to delay treatment or may have other children to raise or other reasons to make that decision). Typically, such a difficult decision would have to be made between 14 and 20 weeks gestation. The circumstances for when a late term abortion is necessary are so limited that they almost never happen. I have, in fact, never seen or heard of a single case of a late term abortion being performed in my nearly forty-year career as a medical professional. The political drama surrounding the concept is completely unsupported by the facts. The determination for the need of such a procedure should be only in the hands of the patient and her physicians.
Why am I writing all of this? Pregnancy is complicated and not infrequently dangerous for the mother, and in general, most people do not understand the process of reproduction and giving birth. They have no idea of the details – the physiology, the anatomy, the developmental embryology (how a fertilized egg turns into an embryo and then a fetus), the changes in the body of the mother, or the process of giving birth. They also don’t understand the meanings of the medical or biological terms that are used. Education surrounding reproduction in the United States is awful, a fact that has seriously contributed to the circumstances we now find ourselves in. If laws surrounding pregnancy are necessary, they have to be informed by science and based on facts, not assumptions, misrepresentations, or beliefs, all of which are all over the map and useless when it comes to making solid objective decisions. From my perspective, the government has no capability or legal standing to have a say in pregnancy matters at all. And neither does an individual outside observer or any group of people. It’s a personal matter that requires the input of a qualified physician and perhaps the input of a trusted religious advisor, a social worker, or a therapist.
Women are in a dangerous situation in the United States due to legislation designed to harm them during pregnancy. I am puzzled as to why legislators who write bills that are meant to directly interfere with patient care and physician decision making, which endanger the lives of women, are not being criminally charged for practicing Medicine without a license. Some women will die or be seriously injured as a consequence of these laws. Legislators and governors who write, support, and pass such laws are guilty of aiding and abetting the death of any woman who dies as a result and should be criminally charged. Unfortunately, there is no accountability for the politicians who are killing and maiming pregnant women in states where legislation has been passed to make life difficult for them. I firmly believe that politicians should be held accountable for the consequences of the bills they write and the laws they pass.
Because some laws restricting abortion seem to confuse a spontaneous miscarriage with an induced abortion, physicians have delayed interventions during and after miscarriage to avoid the risk of being accused of breaking the law and being thrown into prison. Surprisingly, legislators who support abortion bans are blaming the doctors for failure to intervene in a timely manner in these cases, claiming the doctors are at fault for not being courageous enough to take that risk. The legislators claim the doctors are guilty of malpractice if they don’t intervene soon enough to save the mother, but the legislators claim to be guilty of nothing in spite of their legal interference with the physician’s decision-making. Granted, it is up to the physician to decide when intervention is required but given the choice between a malpractice suit for waiting too long to intervene and a prison sentence for intervening too early, well, you’re damned if you do and damned if you don’t. This is the impossible position in which some of these laws have placed the doctor. In twelve states, charges can be brought against doctors that result in significant prison sentences, fines, and loss of the license to practice Medicine. That could, under certain circumstances, be the thanks they get for saving the life of a mother. And even though the doctor is held accountable to make the correct call at the correct time by the legal establishment, the doctor is not considered to be their own expert if a prosecutor brings charges against them. Rather, a Judge (also not trained in Obstetrics and Gynecology) and a panel of “experts” who were not present at the time of treatment and did not examine or talk to the patient are deemed to know more than the treating doctor about what should have been done. It is they who determine the doctor’s fate.
This situation is untenable. Doctors have been put between a rock and a hard place by bad laws, and patients have been put between a rock and a hard place regarding family planning, as they’ve lost control of the management of their own bodies and families.
One might easily predict the outcome of all of this. Many women are deciding not to have children at all rather than risk dying in the process of trying. Many men and women do not want to raise any daughters who might die as teenagers or adults as a result of foolish anti-abortion legislation. Many women who have had pregnancy complications in the past but wanted more kids have decided against it due to the added risk of loss of life these laws impose on mothers. Many women are leaving the United States permanently. And now, as expected, medical experts in Obstetrics and Gynecology are discontinuing obstetrics due to their personal risk of imprisonment for treating a patient who needs help. Furthermore, medical students are deciding not to go into the specialty. What does this mean for women in the United States? It means that pregnancy has just become way more dangerous and thus something to avoid entirely. This result applies across the board; pro-life women, conservatives and the religious are in just as much danger as everyone else. If you’re pro-life, you may lose your life thanks to these laws. Ironically, it’s precisely at this time that the men writing such laws are also putting in place legislation that makes it more and more difficult for women to work and maintain their autonomy while trying to force women to stay at home and be “traditional wives.” “Traditional” meaning pregnant and cooking and cleaning all of the time. The combination of anti-woman, pro-fetus legislation with forced cultural change will result in dead mothers, kids without a mother, and dads without wives.
Clinics that provide reproductive care to women have been closing left and right. Women who need to terminate a pregnancy may have to travel out of State. Such travels have been criminalized by some of those same States; they try to track them down by license plate or by using narcs to expose the patient. They file charges against obstetricians in other (safe) States and try to extradite them. All of this is a violation of privacy and a violation of HIPPA – the patient privacy act.
This is my philosophical stance: life does not begin at fertilization. Rather, life is a continuous line that never breaks. Life creates life. An egg is alive. A sperm is alive. So are the people who are making the eggs and the sperm, and they came from an egg and sperm. And so it goes, back in time, one continuous thread. And yes, of course, an infinitesimal number of eggs and sperm have been cast aside over the millennia – lots of literal dead-ends. All those extra sperm and eggs – an ocean of them, all potential people, had to die so that every once in a while, two could create just one life to maintain the line. Men dispose of five hundred million sperm with each ejaculation, all potential people. Women use up ten or so eggs with every menstruation, with all but one being reabsorbed by the ovary. All those potential people are not allowed to live every month. This is the result of how we were designed. A lucky single egg nominated to go down the tube may or may not meet a sperm it can get along with, and if it does, the resultant fertilized egg has less than a perfect chance of developing correctly or implanting in the uterus. If it doesn’t, it goes out with the menstrual blood. If it does implant, it still has a 30% chance of failure to produce a successful pregnancy due to the risk of miscarriage. This is basic biology.
If one is religious and thinks that life begins at conception, and that every fertilized egg is as important as an already existing human – such as the mother – then one is left to wonder why God thinks nothing at all of wasting eggs and sperm or of killing so many fertilized eggs, embryos, and early fetuses. It has to be intentional, if one believes that God is in charge. Would God murder children? Yes, He would. He did it all the time in the Old Testament Bible and in the Talmud and the Koran. He even ordered people to murder their own children. And other people’s children. And babies! By the way He designed the human body to work, He made sure of His plan to end most lives before they even get started, beginning with the sperm and eggs, and then moving on to fertilized eggs, embryos, and fetuses.
And this is true throughout nature. Other animals function reproductively in the same manner, wasting tons of sperm and eggs and losing a high percentage of embryos, fetuses, and babies. Plants produce gazillions of fertilized eggs – seeds – hoping for one out of a million to make it to adulthood to bring life to the next generation. This is how it is on earth. To have even a single life make it, millions and millions of potential lives have to be cast aside.
Today it is possible to make an embryo from any cell in the body by turning it into a stem cell. A stem cell is pluripotent – it can develop into any type of tissue for which it is genetically programmed, including an entire organism, given the right circumstances. Every time you scratch your back you kill billions of potential clones of yourself. Just think about that. Taking this line of thought to its natural conclusion, the only way to completely stop potential human babies from being destroyed is to kill ourselves. Break the thread of life. That’s how you stop miscarriages, abortions, ectopic pregnancies, and other complications of pregnancy – get rid of everyone. Only then will the loss of “possible lives” cease.
I have a certain practicality about the way I view reproduction and its politicization. I think the terms pro-choice and pro-life are purely political, meant to antagonize. The truth is, if one claims to be pro-life, they have to be pro-choice. They can’t claim that a fertilized egg matters more than the mother who is housing it. It doesn’t. They can’t claim that a fertilized egg is the same as a new-born baby. It isn’t. A fertilized egg is the size of the period at the end of this sentence. It is a potential human, yes. An actual human, no. Over 99% of the people reading this article would not be able to identify a human embryo up to ten weeks gestation if it was placed in a lineup with embryos of dogs, cats, whales, dolphins, cows, chickens, or even fish. Human embryos, like all embryos, go through a period of differentiation, that is, a gradual progression of development that finally ends with a recognizable appearance. If you wait a few days or weeks, you’ll be able to tell the chicken embryo from the human embryo, and vice-versa. They look the same through the initial stages of embryological development.
For humans, it’s ten weeks before you have a tiny human replica in place of the former embryo. It is fully differentiated now, with all its rudimentary organs and parts in place, measuring just one-and-a-quarter inches, and now all its organs and parts need to grow and mature to get ready to live outside the uterus in thirty more weeks. Modern Medicine allows some wiggle room nowadays, so any fetus that makes it to 23 weeks has a fighting chance at life, and any that get to thirty-two weeks before delivery are almost assured of a normal life without consequences. Modern Medicine has made this possible.
The technological advance of in-vitro fertilization has, for some, created another layer of religious, moral, and ethical conflict. To do in-vitro fertilization, you have to give the potential mother hormone injections to cause multiple eggs to “ripen” at once. Those eggs are then removed from their follicles (a little sac of fluid) on the ovaries with a tiny suction device. As many as twenty eggs or more can be removed at once in this manner. Once successfully captured, each egg is fertilized using one healthy looking sperm. The sperm is pulled into a tiny pipette, a glass tube with a pointed tip, and the tip is pushed through the egg capsule and the sperm gently flushed into the egg. The sperm meets the nucleus of the egg, and ta-da, fertilization occurs. The fertilized eggs are allowed to divide in a nutritious broth for a certain number of hours, and the resultant ball of cells (blastula) can then be tested for genetic abnormalities and frozen for later use. Many, if not most, of the blastulas/blastocysts will not survive long enough to be frozen for later use. Some will have genetic abnormalities that prevent use. Once the potential mother has been properly prepared with hormones to maintain a pregnancy, one of the remaining healthy blastulas/blastocysts can be carefully placed inside the uterus, again using a pipette. Most of the time they take initially, but again, the miscarriage rate is similar to the rate for a natural pregnancy, so often the mother will have to go through more than one cycle to finally have a successful pregnancy.
Sometimes there are frozen blastulas/blastocysts remaining in the lab after the parents have completed their family. They can’t be kept forever, and at some point, they are discarded. The little balls of cells can barely be seen with the naked eye, but some people seem to think they are the same as a person. They are not. Yet, they want laws to force the labs to keep the blastulas frozen forever. They will never be used, and eventually, they will perish regardless of being frozen, so such laws are not only useless, but from a practical standpoint, ridiculous.
The science behind the development of a life is vastly complex. I am always so surprised at how quickly a human creates itself considering that complexity. And it does create itself; it is genetically programmed to make itself into a human from a single beginning cell. The process is astonishing. The mother’s job is to stay healthy and prepare for delivery as that cell turns itself into a little person. She is not doing anything directly to get it to develop, it just does it, as long as nothing is awry. It is nothing short of miraculous that a cell can do that, or that a mother’s body can change enough in the process to accommodate it and then bring it into the world. Afterwards, the mother will never be the same as she was before. She is permanently changed.
In conclusion, I do not think congress or any legislature should have any say about how anyone manages any health issue, and certainly not how women manage their pregnancies. The medical and biological sciences fields have thoroughly studied the pertinent issues, and it is their recommendations that should be followed. If a gestational date is set beyond which deliberate pregnancy termination should be considered inappropriate, that date should be determined by our many national pediatric societies, the American Society for Reproductive Medicine, and the American College of Obstetrics and Gynecology, with recommendations for exceptions determined. These should be solid guidelines, not laws, taking into account that each situation is unique and that the government does not have the professional expertise required to be making such decisions for the patient. In fact, it should be against the law for legislators to “dabble” in Medicine while in office. The clinical application of health care must be in control of the experts who undergo upwards of twelve years of intense education to become capable of taking care of a human being in times of medical need. They are experts who have dedicated their entire lives to women’s health. Complicated matters such as these can only be properly managed by the patient and their medical advisors.

I don’t like being a patient. Never have. I just don’t have time for it – I have much better things to do than have something wrong with me. That said, as a rule, I am a “good” patient when I have to be one. I have my own opinions about how active a person can be after surgery, though, so I don’t usually follow the “rest” directives given by the surgeon. I’ve always thought the quicker one gets back on their feet, the better – being a bit careful, of course.
My first major experience with the medical system was at age 19 when I had an open appendectomy. I was filleted like a fish by an old general practitioner in a rural hospital. He had a senile tremor, so his hands shook like a leaf. I wondered how he could work on me with such shaky hands. Afterward, we had a battle because the doctor said I had to drink before they would discontinue my IV, but I was peeing every five minutes because of that IV. I told him I wasn’t drinking a drop until he removed the IV – my bladder was sick and tired of working so hard. He doubled down and said he wasn’t going to remove it until I drank. So, there we sat, butting heads. I told him I’d take the damned thing out myself. My mom was sitting there and was horrified that I was sassing the doctor, but I didn’t care. I got up and marched to the bathroom to pee for the millionth time, gown wide open, ass fully exposed, further freaking my mom out. Finally, I talked the nurse into giving me one glass of juice in exchange for removing the IV. We compromised, I guess. We all felt like we won. I was stuck in there for a good five days. I was ready to leave at two! As soon as I got out of the car at home I went straight to the barn where my dad was roofing, climbed up the ladder, and started nailing in the corrugated tin panels. It hurt a bit, but I was careful, and I wouldn’t have had it any other way. I got better quickly, and I think it was because I decided to get up on that barn. It was a sign of my attitude toward being laid up.
Years later a disc ruptured in my lower back while I – now a doctor – was in the middle of performing a major operation on a patient. There was no one available to take my place, so I simply had to grit my teeth and keep working in spite of the severe burning pain going down my leg. I finished the case and went straight to radiology for an urgent CT scan, followed by an urgent epidural injection to provide some pain relief – it was bad. Two days later I had an urgent partial discectomy with facet bone removal. The next day I woke up with a mostly paralyzed right leg. “Well, shit,” my neurosurgeon said when she made rounds. “This almost never happens.”
At least my pain was gone, what a relief. “Will I get better?” I asked. “I don’t know,” she said. “Either you will, or you won’t. Time will tell.” I was just 44 years old. “I’m going home then,” I said, and off I went, less than twenty-four hours after being admitted.
I had no time for having a paralyzed leg, I decided. My son bought me a dragon cane while I was away, and he happily presented it to me when I got home. There was a sword inside. Good! A weapon, just what I needed to fight off infirmity.
The leg wouldn’t work. I swung it around enough to use it as a sort of peg-leg, like a pirate, using the dragon cane when necessary. I was neither happy nor sad, just bemused, even though it appeared my career in surgery might well be over. I studied the leg as I traversed down the stairs the next morning to get coffee. “Stupid leg,” I muttered to myself.
I went to the gym the next day and gimped around, even though the neurosurgeon had told me I had to wait three weeks. I tried out the leg extensions. I normally could do 150 pounds per leg on that machine, but now I could only do 5 pounds with the right leg. I had almost no working quads, and my glutes were weak as well. I managed to do most of my regular workout in spite of the leg. The next day I did the same, and the next day, and the day after, and little by little I began getting some strength back. I waited six weeks, and then went back to work, first just doing easy things like scopes and hand surgeries. Over the next year I gradually got back to all of my normal work, albeit with half the hours and with accommodations in the operating room. I ditched the cane after the first six weeks. I willed my leg to work, kept my posture as perfect as possible, and tried to walk smoothly like a dancer everywhere I went. It was slow going, but after two years I had only a barely perceptible limp.
And then the disc partially ruptured again, assuring my fate of never getting completely better. I modified my work schedule permanently then and kept going anyway. People needed me.
Other things have happened, other surgeries, other conditions. Doctors are not immune to illness. By the time I was in my early sixties, I just had to stop being a surgeon. It was the combined stress of my career, not just the physical stress that led to that decision. I was physically and spiritually exhausted. Within months of retirement, I looked and felt better than I had in over a decade. My boys thought I had aged backwards. That’s over now, I think – one can only age backwards for so long.
I’ve had bad experiences as a patient. Not with actual treatments, but with providers. The first time was with the appendectomy when my doctor wouldn’t listen to me. He was making my bladder explode and wouldn’t consider my viewpoint. I was just a dumb farm kid, after all. “The doctor knows best.” The second time, though, I was 57. I needed a heart catheterization, having unfortunately inherited my dad’s predisposition for coronary artery disease. I was sent to Mercy in Des Moines for this procedure, to be performed by an interventional cardiologist who I had heard of but never met. The nurses prepped me in preop and said the cardiologist would be by in a few minutes. He appeared, picked up my chart, confirmed my name, looked at the indication for the procedure and simply said “We’ll be starting in a few minutes.” That was it. No greeting, no introduction, no opportunity for questions – nothing. I could tell he had not bothered to look at my chart until just that minute. He turned to walk away. “Hold the phone!” I said. “I have some questions.” He turned, exasperated, but didn’t approach the gurney. I then proceeded with my questions, one after another. Pretty soon he began to get the idea that I was more medically savvy than most of his patients, but he remained irritated. Had he looked at my chart, he would have known that I was also a physician – but that fact shouldn’t have made any difference on how he treated me. His failure to engage me properly from the start was a grotesque example of how doctors should not behave. After a bit, due to his obvious ongoing irritation, I finally told him I was also a physician, and then all of a sudden everything changed. He pulled up a chair and sat down, finally, and managed to hide his annoyance and have a conversation with me. But I told him exactly what I thought about how he had presented himself. He replied that he was the best invasive cardiologist in the Midwest, as if that should be qualification enough to allow him to be an asshole to his patients. I wasn’t having it. “You will sit there and answer my questions until I am done,” I told him. “Otherwise, I am taking out this IV and walking out the door.” So, he sat there while I tortured him with questions. He squirmed the whole time.
This should not happen to any patient. I moved recently, and now I have to find all new providers. The whole system here is different, with lots of emphasis on specialty treatment rather than management by family physicians. The care is fragmented and there are too many appointments to deal with. And three times now, with different specialists, I’ve been talked to as if I’m an idiot, been hurried through the appointment, and given wrong information to boot. And once again, no one asked me any questions to figure out who I am. They just made an assumption based on the diagnosis that was used to justify the appointment. It’s as if I am just a diagnosis, not a person. I let them go on for a while at each appointment, just to see how long it would take them to figure out they were being judged, but they never figured it out. After about five minutes, in each visit, after correcting various mistakes they were making about my diagnosis and reason for being there, I finally said, “I’m a physician, you know,” knowing that they didn’t know. And then all of a sudden, they listened to me and what I had to say about my past and current medical history and why I was there. In every case, they had it wrong until I corrected them. These were Harvard, Yale, and Stanford doctors. The best, supposedly.
The proper way for a doctor to enter a room and greet a new patient is with a smile, an introduction, and a query about why they are there. They should already have reviewed the patient’s chart and already know the answer, but they should hear it directly from the patient. Then, the doctor should say, “Okay, we’ll get back to that in a minute, but please tell me a bit about yourself. I want to know about your background, education, career, and family.” This sets the tone right away for rapport and trust and indicates to the patient that the provider is actually listening and recognizes that who you are matters. Once the provider knows more about the patient, they can tailor the interaction to fit the patient. I cannot emphasize enough how important this is!
From now on I am simply going to tell the first person who takes me into a room that I am a physician. I shouldn’t have to do this, and it makes me wonder how in the world do non-medical people manage at their doctor’s office or at the hospital. I think it’s safe to assume that many patients are being talked to as if they are children.
I know I wasn’t a perfect doctor. Some days I was definitely crabby or impatient. One day a patient complained to my nurse that I had failed to introduce myself when I came into the room. I had assumed it wasn’t necessary; who else would I be if not the surgeon they came to see? I realized I shouldn’t make such assumptions; I’m just a man. I could be a nurse, an assistant, a tech – how would you know? A nametag would help, but what if the patient has poor vision, or the tag is obscured? They shouldn’t have to even think about it! I should have introduced myself. But I would like to think that the vast majority of the time I took a minute to introduce myself, touch bases with the patient, make sure the chart documentation was correct, make sure I was accurately understanding their report, and assuring them I had understood the problem and understood them as a person. This seems like it should be the bare minimum for a doctor’s appointment.
Another problem is appointment frequency. I have a new cardiologist. She seems great. But she wanted to make another appointment to see me in six months after our initial visit. It’s a three-hundred-dollar follow-up appointment. I told her no – I would see her in a year. It’s been nearly three years since I had heart stents placed, I have no new symptoms, by blood pressure and EKG are normal, and my exercise tolerance has steadily improved. What was the point? What will she do if I’m just the same then as I am now? “Nothing,” she replied. “So, I would be paying for a “nothing” visit, an unnecessary visit. I could make the argument that even a visit at a year is unnecessary if I’m feeling well,” I said. She pondered my observations for a second and then agreed. “You know your body,” she said.
I also know my pocketbook, and like most retirees, I have to keep an eye on it. It can be expensive to go to the doctor even with insurance. And beyond that, I don’t want my world to revolve around doctor’s appointments. What sort of social life is that? I see my dentist four times a year, the Ophthalmologist twice per year, the optometrist once per year, the endocrinologist twice per year, the cardiologist once per year, the primary care doctor once per year as a routine. On top of those eleven visits will be others, such as urgent care for an unexpected illness, the dentist for filling a cavity, the pharmacist to pick up meds, or any number of other providers due to the development of some other new symptom that has to be chased down, and I’m in relatively good health for a guy my age! I would say I will be lucky if I have only twenty medical visits per year! In my younger years, from age five to forty-four, I saw only an optometrist annually. I saw a primary care doctor only once every few years. The older people in my practice often complained to me that “all they ever did anymore” was go to a doctor’s appointment. I totally believe them.
I often thought about the imposition of loss of time and money on my older patient population due to doctor appointments. Some couldn’t drive well. Some couldn’t afford gasoline. Some were disabled, making it difficult to arrange transportation. This always bothered me. As often as possible, if someone called in with a question about their health, I would take care of it over the phone. If they had a problem other than the surgical one I was seeing them for, I would take care of that as well to save them a trip to another provider or urgent care clinic. I would often set up phone appointments, and later in my career, video calls so the patient would not have to travel to see me if it wasn’t absolutely necessary. I even made house calls and nursing home calls on the regular for consults, wound care, and so forth. I did whatever I could to make access to health care possible for my patients.
In many ways, I think, practicing Medicine in a smaller environment is so much more practical, as is focusing on primary care. That means that the primary care providers have to be broadly trained and the specialists who work with them must communicate effectively and use the primary care provider to deliver as much specialty care as they can. The specialist should act as a consultant for the patient initially and then as a guide for the primary care provider as much as possible. Visiting specialists can certainly make a difference too for patients with transportation, financial, or disability issues by coming closer to where the patient lives.
The model we used at UnityPoint Grinnell Regional Medical Center in Grinnell, Iowa, was – in my opinion – nearly ideal. Almost all the doctors/providers lived in town, and everyone who lived in the region knew who they were and often saw them around town. We had a common community, and we answered to each other. The model was primary care focused, with general specialists in-house, and visiting subspecialists coming in on a regular basis. The providers were easily able to access the general specialists in their clinics, and there was a sense of camaraderie amongst them. Since we and the patients all lived in the same town, we had to answer to each other. I don’t know exactly how to translate that into an urban environment, but I’m appreciative of those who are thinking about it and trying new things, like video appointments. Meanwhile, I’m very grateful to have had my career in Grinnell. What a great place to work! Just the right size, and great people all around who understood their mission and their role in the community and hospital. Everyone in the Grinnell area should be very proud of their little powerhouse of a hospital and the caring staff and providers who work there. The place is a gem. Or, ahem, for those in the know – a jewel.

You have to admit, this is a very weird looking tree, the Baobab. There are six species in Madagascar, two in Africa, and one in Australia. They inhabit flat, arid, low-lying regions. The trunk of this tree can absorb and hold an enormous amount of water for an extended period. The trees are deciduous, as they lose their leaves and go dormant for part of the year during the dry season, which starts in the fall and extends over the winter in their native lands. They have long lives – over a thousand years potentially. They can only grow in deep tropical environments, as even a temperature of fifty-four degrees F is too low for them. Mythologically, the story of how they got their peculiar shape is that “the devil plucked the baobab tree out of the earth, turned it upside down, and jammed it top first back into the ground, leaving the roots in the air.”

Above is a young Baobab tree in a Bonsai pot. Here, in miniature, it is confined and has grown into a tiny version of the regular enormous Baobab that exists in the wild. I think it is an interesting tree visually in either form. I’d like to have a Baobab, but the only way I can possibly do it in Connecticut is in the form of a Bonsai.
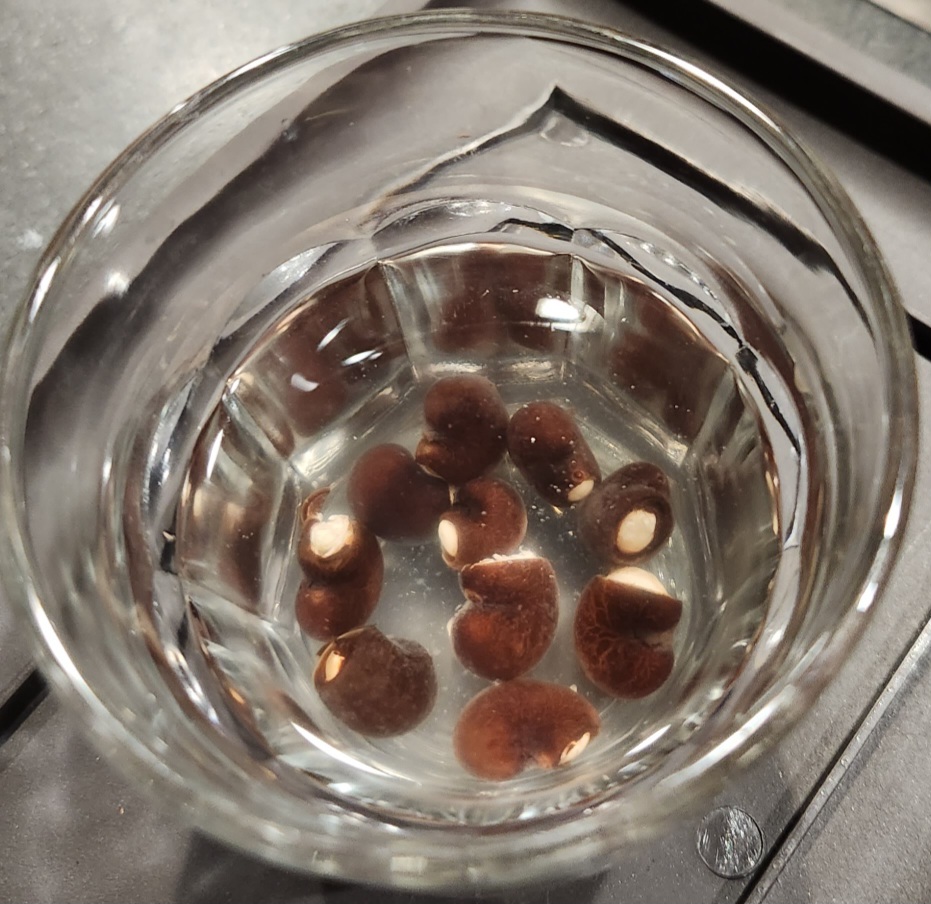
So how can one get a Baobab tree to Bonsai? Well, you can order seeds online, much to my surprise. They are typically shipped in a bunch of ten, as a percentage are duds and the initial survival rate for the seedlings is only about one in three. To find the duds, the seeds are poured into a glass of water; those that float are no good. The remainder are kept.
The process of getting the seed started is complicated, as the seeds of the Bonsai are as strange as the tree itself. Each seed has a black, thick, hard coat surrounded by a second softer brown coat. It takes a long time for the seed embryo to work its way out of the outer hard coat to germinate, months and months, and only when the conditions are just right. This is too long a wait for most people to tolerate for a specimen tree, so a way was found to force germination much more quickly. The process requires soaking the seeds for three days in a glass of water, then filing or cutting the seed coats back on one end until you can see a small sliver of the white seed embryo. Then you put it back in a glass of water for 2-3 days during which time the seed will swell and soften from within, thanks to the hole in its coat. Below is a photo of my soaking Baobab seeds. I used a Craftsman wire cutter to nip off the seed coat to expose the white seed interior before putting them in water. They began to swell quickly, and after two days they were ready to peel, using my thumbnails. Quite easy, really.
Below are the baby tree embryos which have been removed from the seed capsule. They will soak for one more day in this bath before transfer. One end of the embryo is a pair of cotyledons – the leaf like structures that open to feed the new tree as it sprouts. You see them on beans when they first come up, so I know you’re familiar with cotyledons even if you don’t know what they are called. On the other end of the embryo is the root stub. The embryos began enlarging almost as soon as they were released from the seed hull. As you can see, they look weirdly like insect larvae, or grubs.

After soaking for a day, the embryos are placed between layers of moistened paper towels in a warm place in the house for another 2-3 days or so, during which time they begin to sprout. Once the little root is seen and the sprouting embryonic leaves are reaching up, the baby is planted an inch deep on its side in moist potting soil and kept in a warm place. Within fourteen days, the two leaf-like cotyledons will emerge from the soil, followed soon by the new growing stem of the tree. In the photo below you see the two big leaf-like cotyledons, and between them, way down deep, just the hint of two tiny new leaves coming up on a stem.

This little baobab tree is in a “training” pot made of plastic. Training includes regular root and branch trimming, and when necessary, wiring of the branches to make the tree look like the sculpture you want. When it is bigger and more well established, training will begin, and eventually it will be transferred to a larger and deeper ceramic pot where it will live permanently.
If my bonsai experiment works out, you will see new photos as the tree develops. In the meantime, I will be trying bonsai with other types of native and ornamental trees from the Northeast. Hopefully I will have a cool collection soon.

A slave cannot have two masters. This is a truism.
As a surgeon, my master was my oath to always put the medical needs of my patients first. Not the hospital’s needs, not the clinic’s needs, and certainly not the insurance companies’ needs.
By law, in order to be licensed, a physician of any type must remain up to date with educational expectations and practice to “the standard of care.” The standard of care is what most physicians in any given field would do for any patient with a particular diagnosis, taking into account that each patient is different than the next. Physicians are obligated by law to hold to this standard, not just by moral conscience.
So, what are we supposed to do when an insurance company, like United Healthcare, does not have the same moral center or sense of obligation to its clients? What are we supposed to do when United Healthcare consistently refuses to approve necessary surgeries, medications, and tests?
I retired almost three years ago. When I left, automatic denials of physician submissions for approval for medically necessary surgical care was the norm for United Healthcare. It was always safe to assume that whatever the patient needed, United would turn it down. In the cases they didn’t, they might retroactively turn it down and demand return of payments made. Yes, that is correct. “Upon review of the case, our reviewers have determined that the patient did not meet criteria for surgery for their condition and therefore you have ten days to return payment for the procedure done.”
So, not only does United block access to medically necessary surgical care, but they also will take money back for the work already done by the surgeon for medically necessary surgical care. Both of these situations are so common that it has become a joke. Except that it’s not funny. United Healthcare profits in the billions by refusing to do the one job it has been assigned, and that is to honor their contract to their patients who need physician approved care.
What does this do to the physicians? I will tell you. Every day, all day long, we are faced with one difficult medical/surgical patient after another, all of whom expect us to put their lives first. We are, after all, the experts. We teach, we advise, and we move quickly when it’s necessary to prevent death or disability. So, imagine trying to do this, knowing that you are the expert, Board Certified in your specialty, only to have your patient’s medically necessary surgery cancelled by the insurance company. All day long, this goes on. It sucks the life out of the clinic nurses and the surgeons trying to take care of the patient. We have a patient on the table ready to go to sleep for a major case, and then we get a phone call from our nurse saying that we need to do a peer-to-peer review of another case because payment has been denied. We need to be focused on the case at hand, but now we are distracted by the insurance company.
And let’s talk about “peer-to-peer” review. It is supposed to be a conversation with another physician who is also Board Certified in your area about the patient’s care. But this is not what happens. Instead, you get a general internist or a primary care physician on the line, not a surgeon. And they argue with you, even though they are not an expert. And they have the final say rather than the surgeon who has been taking care of the patient. The peer-to-peer insurance company consultant has not examined or seen your patient, nor have they talked to them. They have not reviewed the radiologic studies with their own eyes. Frequently, they have not even bothered to review all the details in the reams of pages of information my office staff sent them to support the decision for surgery. Not once, in my thirty-year career, was an insurance company decision not to pay for a covered patient’s surgery correct. Not once! And yet, as the years went by, I was hassled more and more and more by this system. The emotional toll taken and the stress caused by this never-ending onslaught from United Healthcare was disastrous for my sense of well-being. Every denied case turned into a fight between me and United Healthcare. Every day I had to put on my emotional armor to go to war, it seemed.
A physician cannot be both a slave to their patient and a slave to the insurance company. We have already chosen our master, the person we are committed to supporting no matter what. We cannot be slaves to the business of profiteering that United Healthcare has so fully embraced.
What about other health insurers? Anthem could be a problem at times. Iowa Blue Cross/Blue Shield had a very good system and rarely interfered with the care I needed to deliver. Principal went through a phase in the 2000’s where they were instigating internal investigations of any surgeon who performed “too many” specific treatments for certain conditions. I was targeted by one of these investigations because I was by far the busiest surgeon in Iowa in the treatment of gastroesophageal reflux disease. I was the busiest because I was the most expert, but that didn’t stop them from trying to find a way to blackball my practice. I found out they were doing this investigation by accident while trying to get to the bottom of a decision they had made not to cover a case. So, I had to get an attorney involved to get them off my back.
This sort of thing wears the surgeon down. It wears the case managers down. It wears the nursing staff down. And it is extraordinarily damaging to the patients emotionally and psychologically.
Twice I had cases that I could not get approved. Only twice. But that’s because I would never accept “no” for an answer. I was highly expert in my field, and I just wouldn’t put up with it. I was incredibly aggressive about holding the insurance company to task. If they assigned a non-surgeon as my peer-to-peer, I would demand they find a surgeon to talk to me, someone who understood my specialty. If they had not done their homework and reviewed all the information sent in to support the case, I would rip them apart for not doing their job. I would also question their ethics and morals and ask them who had advised them to routinely refuse approvals. I would torture them as much as they were torturing me. I told my patients to write letters to them and get attorneys to write letters. They were wasting my valuable time, so I wasted theirs in return.
Yesterday I saw a video of a young surgeon who decided to quit surgery entirely because of the ongoing “moral injury” she was enduring from knowing her patient’s needed surgery and not being able to get their surgeries approved for payment from United Healthcare. It put her in a constant state of anxiety and distress to know that she could not, because of the insurance company, do her job and uphold her commitment to “do no harm” in her job. This is entirely unacceptable.
The entire practice of prior approval should be completely discarded. It is nothing more than a mechanism to deny and delay care and maximize profits for capitalistic health insurance companies so their investors can be paid handsomely and their CEO and business managers can financially rape the system for personal financial gain.
We are way past the point when health care should have been overhauled in the U.S. No one should have to be worried about being bankrupted by the insurance companies or denied care. No one should have health insurance that is tied to employment. No doctor should have to put up with abuse and manipulation from the insurance companies. Health care should be available to all whenever it is needed, period. It should be broadly government supported. And all private health insurers should be not-for-profit. Medicare should have been made the national health care insurance program for everyone when it very first began, starting with birth.
The patients are furious and so are the clinicians who are actually doing the work of healing the sick while being constantly harassed. Clinicians need to rise up as one and demand immediate change and fight for every patient like a tiger, and congress needs to take this problem seriously, stop the politicizing, and fix it, once and for all, making it impossible for private insurers to be running the show. When a patient is sick, you never hear them say, “Is there an insurance company CEO nearby who can help me,” do you. Nor do they ask for a business manager. Nor do they ask for an insurance clerk. They ask for a DOCTOR, and rightfully so.
Health insurance companies, get out of the way. Everyone is sick of you throwing up roadblocks to the delivery of patient care. Where is your ethical center? Where is your moral center?
And congress – how nice that you’ve arranged for nothing but the very best healthcare for yourselves while hanging the American people out to dry. You’re just as bad as United Heathcare and you’re not doing your job as public servants on behalf of the American people. Step up for once in your lives and do the right thing and solve this problem once and for all.
I have been baffled for over a decade now about why we have failed to talk about the simplest solutions for global warming. I am referring to planting trees and completely protecting all existing tropical and temperate forests and avoiding black surfaces for buildings and highways. These are three simple things that could already have been implemented to good effect while awaiting the more difficult technological solutions, such as optimized electric cars and solar and wind energy production and alternative fuel sources such as hydrogen.
I am even more baffled about all the talk of sending men to Mars or the moon and starting colonies there to “save” humanity. That isn’t going to happen. Humanity can’t even take care of itself on the planet upon which it came into existence, a planet that was perfect for us until the past hundred years! We’ve ruined it. How do you think an enclosed Martian or lunar colony is going to “save humanity” in a place with no breathable atmosphere, temperatures below -200 degrees, low gravity, and dangerous radiation levels from the sun? Humans cannot survive for long in such conditions, even if a habitat was built. What makes us think we can transform another planet to perfection for humanity? It’s a joke!!! The only way humanity can save itself is to attend to the earth as if it is the only thing that matters. The only way that can happen is if everyone on the planet gets on the same page and sees the earth for what it is – the only safe place for us.
So what are the simple things that can be done?
- Create world laws and treaties that halt the destruction of all forests and activate plans to re-establish lost forests. Forests are the lungs of the earth. They absorb massive amounts of CO2 and they do it with zero effort. They are responsible for oxygen production, which we cannot live without. Without forests, every living thing on the planet will perish. Likewise, stop destruction of ocean ecosystems. This means stopping pollution and overfishing. Ocean plants and algae are also major sources of oxygen and have to be protected. Remember – the earth is an island, floating in the vast sea of space. There is no place to go to get more oxygen, or to get rid of CO2 – the earth was doing it just fine until humans foolishly decimated the world’s forest ecosystems and totally raped the environment. Like you, the planet cannot live without its lungs. It can’t breathe.
- Governments should set aside funds for tree planting throughout cities and towns and re-planting them in forest areas that have been decimated by agriculture and logging industries.
- The human population is twice as high as it should be. Everyone should agree to reduce reproduction rates for the sake of the whole – it’s a moral responsibility. This is no time for selfishly having large families for personal gratification.
- Re-paint black, dark gray, and dark brown surfaces lighter colors, such as white, tan, or light grey. Stop the production of dark colored roofing materials. Houses, highways, and cities are heat sinks, adding to global warming.
- Seriously take steps to eliminate all sources of pollution so the earth can heal itself.
- Change our agricultural practices to sustain the environment and protect fresh water.
- Stop spending money on weapons and war and turn it instead to science-based education and saving the planet.
If every person on the planet took the preservation of earth seriously, we could prevent the looming humanitarian catastrophe that is about to occur. As it is, there WILL be a sudden, massive die-off of the human population soon, along with nearly all other species of plants and animals. The process of mass extinction is already advancing quickly. This is what always happens on an island where resources have been decimated and the demands of the population continue to outstrip the ability of the island to provide.
What I am witnessing in society now is a sort of manic self-destructive response to the threat we are facing. Instead of slowing down and making educated changes in how we live and take care of our planet, we have – as a group – accelerated the destruction of it, living as if there will be no tomorrow, and thus guaranteeing our own demise. More cars on the road, people driving as fast as they can like maniacs, people frantically travelling the world to meet their bucket lists, governments encouraging more fossil fuel harvesting, politicians destroying environmental protections and eliminating or rolling back air and water protections, billionaires sucking up space and resources to show how big their egos are by shooting off giant rockets and sucking up millions of gallons of fuel and spewing the resultant pollution into the atmosphere, more drag-net fishing, more people advocating for big families and fewer birth control options, and on and on. It’s as if everyone has lost their ever-loving minds. We are all individually responsible for the welfare of our planet. It is not just the government’s job. We each have a moral responsibility to the earth and all of its inhabitants, human and non. We are not living up to it.
So, what can we do as individuals? Anyone with even a small amount of land can plant trees, shrubs, and herbaceous plants. Native trees can often be obtained from agricultural universities at minimal to no cost for planting. Even an apartment dweller can help by keeping potted plants/trees on their deck or balcony. Lawns can be converted into botanical ecosystems. We can choose to put light-colored shingles on our homes when we re-roof. We can stamp black pavement in our driveways with light colored paint. We can tap into government funds to put solar on our home or business if it’s amenable for the location. When we get a new car, we can switch to a hybrid or electric. We can use native plants for our specific areas to reduce water demands. We can stop using plastic and promote recycling. We can get more involved in local government where grassroot movements can flourish.
The big projects can only be done and funded by governments, but if two or three trees were planted around the world for all individuals who exist – 24 billion trees – 720,000,000,000 pounds of carbon dioxide would be taken from the atmosphere annually once the trees are medium sized. Likewise, 24 billion new trees would produce 2,080,000,000,000 pounds of oxygen. Two medium sized mature trees can provide enough oxygen for a family of four around the clock. But other plants remove CO2 and produce O2 as well, from single celled plants and algae to herbaceous plants and shrubs. So, planting gardens and re-establishing botanical ecosystems on land and in water everywhere should be done. And individuals can do this in their own space! Instead of going out to dinner some evening, buy a tree. Plant it! Take care of it! Then plant another one!
I am writing this because it seems on the surface that individually we are helpless to do anything about the collapse of the planet. Some countries are doing a great job from a government standpoint – they are doing all the right things to help. But those which are having the biggest detrimental effect are not pulling their weight; I’m talking about Brazil, the United States, and the tropical countries of central Africa and Asia. The U.S. has taken an antagonistic approach to saving the planet. Conservative American politicians seem to want to hasten its destruction, and at least some of our American citizenry are being deliberately obtuse about their individual responsibility to take personal action. Change starts with the individual. There are a lot of individuals in the world, enough to hold the power to change the seemingly inevitable result of our stupidity of the past one hundred years. It’s time to wield it.
I wish I could start a world-wide “Green Movement” of billions of people who are willing to look at the big picture, step up to the plate, and just do what they can do individually. With enough individuals choosing to do the right thing, no destructive government policy or law could overwhelm the good that the people of the world can do if they decide to.

It took us a long time to find an ideal place to live here in Connecticut. The biggest issue was a lack of available homes for sale, and competition had both driven up prices and made it nearly impossible to be the lucky person who ended up with a new house. It was normal for twenty offers or more to be in the queue for consideration the very day any decent house was put on the market, and those offers often were in excess of twenty percent over the asking price, and the beginning asking price was already high. To be considered, the offer had to be straight up cash with waiving of inspections and acceptance of an “as is” clause. To add insult to injury, the homes for sale had not, as a rule, been well kept; all had significant delayed maintenance issues that the seller was shifting to the buyer. Take it or leave it.
The sellers seem to lose all perspective and manners in their rush to cash in on the largesse of their home’s value in a market that puts them totally in the driver’s seat. All told we tried to put offers on a half dozen places or more, none of which were in excellent condition. Even those that had been totally renovated had major problems with low-quality materials for construction and a lack of quality workmanship. I couldn’t help but wonder how in the world a young couple could manage in this market. It would be so easy to be duped if you didn’t have personal experience with home or building construction. You wouldn’t know what to look out for.
The first place upon which we placed an offer that was accepted was a little house on two acres with a barn and a little garden shed, located in a fairly remote area. The house was too small, really, but at least the first floor had been decently renovated. To win the contract bidding we had to offer an amount way over the asking price and skip inspections. We didn’t agree with the process but knew we wouldn’t even be considered otherwise. There was plenty of outdoor space for me and my outdoor inclinations, we liked the barn, my doves could live in the little garden shed, the house had just enough space to place Kev’s piano, and the kitchen needed a bit of work but was expansive and well organized. There was not space for a library and the bedrooms were all too small, but we just decided we would have to figure out what to do about that later. The owner of the place was a landscaper, so they had a lot of things to remove from the property. The closing date was thus made three months down the road.
Ten days before closing we flew out to do a final inspection with the sellers, which I insisted upon. The seller had done a lot of work on the place himself, and I wanted him to explain to me how the house functioned, especially all the mechanicals. It was during this tour that I noticed the basement floor on one side of the main room, one wall, and the foundation of the fireplace in the basement had all been reconstructed. None of this was mentioned in the disclosures he had filled out (all foundation issues are required by law to be revealed in CT). He then told me about the years of trouble they had with the basement floor being cold and “sweating” all the time, and how they discovered, when they added a small living room addition to the house, that there was a large underground stream running under the basement floor! He went on to explain how they had “fixed” the problem, though he didn’t really know whether or not the stream was still running under the basement.
I made a mental note about this and finished the tour. Afterward, Kev and I discussed the findings of the day and over the course of about twenty minutes concluded there was no way we could close on this house. That night we cancelled the purchase and explained to the seller’s agent that there had been no disclosure about the river under the house or the foundation work that had been done to mitigate it, thus voiding the contract. We expected our deposit to be returned, but no – the sellers said they would not return it without a court battle. We went back and forth for two months, and I finally countered with a threat to sue them for fraud if we couldn’t come up with a fair disposition of the deposit. This brought them back to the table. The cost of doing battle in court would have consumed way more than the deposit, so both sides gave in a little and we all walked away annoyed with the outcome. They had, of course, sold the place to someone else for the same price the day after we cancelled the contract. They were hoping to make an even bigger profit by keeping all the deposit; and never mind the fraud.
Another place, on the Farmington River, came on the market a couple of months later. It had many attributes but needed a ton of work. It was small. Cool location though, with big boulders and a steep slope going down to the river. It could work. The seller had bailed out of the first contract he got because he said the buyers were “too demanding” because they asked him to fix a bunch of things before they took possession. He had just built a four-million-dollar house down the river a ways, so he didn’t care how long it took to find a buyer that he could push around. He’d left the place a mess. We made an offer taking into account the results of the inspections which had been insisted upon by the previous buyers. It was turned down. The house stayed on the market for three more months and two other offers were turned down. We resubmitted our offer, and the owner accepted it but would not sign it because he wanted to wait just a few more days in case someone else came along with a better offer. It had now been eight months since the house had been originally listed. It was quirky in many ways, had no yard, had a steep driveway, and had only two bedrooms – thus the paucity of offers. We didn’t think anyone would swoop in with a better offer. But lo and behold, three days later a buyer came in with a slightly higher offer and the owner jumped ship and signed a contract with them. So, that was that.
At this point we decided to give up and see if we could find an apartment and just fly back and forth every six to eight weeks as needed to help with our granddaughter, the reason for which we were house hunting in the first place. The next time we went out, we searched diligently and found an apartment we thought would work well. We decided we would put our house in Iowa on the market again in the spring and sign an apartment lease in Connecticut in the summer. If we didn’t sell our house, we would stop searching and just live in both places. If we did sell our house, we would put our stuff in storage and live in the apartment until the housing market was behaving better.
All of this happened between August of one year and January of the next. In February we put our house in Iowa back on the market. There was an initial flurry of interest and one offer, but that failed. The day before we flew out for our granddaughter’s birthday, however an unexpected buyer appeared and made an immediate offer. We signed a contract to sell. The next day, in Connecticut, we had arranged to see two houses with our real estate agent. Neither one was okay, for all the same reasons as usual, plus locations on busy roads. “There’s one more that isn’t yet on the market I think you should see,” our agent told us. “I think it might be perfect for you two. The owner is away in Florida for the winter, however, and it won’t go on the market for two weeks yet. But we can go look at the property and you can look in the windows. I’ve known the owner for many years.” So, off we went, over the mountain and through the woods, and pulled up to a little ranch style house. It was perched on a near-precipice overlooking a little pond, surrounded by massive white pine trees and forest. “I already love it,” Kev said as we leapt out of the car. Our agent knew all about the property. One acre, house built in 1960, renovated in 2006. She’d been in it many times. It was locked, so we walked around and peered through the windows. I could see it needed work but saw nothing that looked serious. It was, indeed, perfect for us. A little room for the piano, an open main floor, two bedrooms, an art studio in the basement that could be a library, and a garage big enough for our little car and the motorcycle. The setting was idyllic, and it was on a long cul-de-sac, so there was no traffic.
And then, there was the garden room. “You have to see it,” our agent said, before we got back in the car. I was imagining some sort of greenhouse with lots of windows. “It has a door without a lock. It’s under the master bedroom.” Strange, I thought, to have a garden room under another room. How would it get light? We walked across the poorly maintained brick patio outside the art studio. There was a deck attached to the master bedroom there with a cement patio and porch swing underneath. A simple door stood there in a blank wall. We opened it and walked in. It was just a dungeon. Cement foundation walls on four sides with just one tiny window high up on the wall in the southeast corner. A prison cell, really. It was cluttered and dusty. Four dim bulbs with individual pull strings dotted the ceiling. We turned one on. Lots of garden tools came into focus, scattered about. A massive bureau was against the front wall. The ceiling rafters and insulation were exposed, as were all the pipes and electrical. Two supporting Lally columns were under a beam going across the middle of the room, one completely rusted. There were spider webs and tv cables snaking everywhere. “The owner’s husband watches a lot of tv,” our agent sighed. “He has at least one tv in every room in the house. Fox News, you know. He can never turn it off.”
I studied this dark, dank dungeon of a room for a few minutes. It was big. It would always stay the same temperature, I knew, being underground on three sides. It opened onto the patio which overlooked the pond and attached to all the gardens. “Perfect,” I thought. A perfect room for potting plants and overwintering dormant plants, perfect for my tools and gardening equipment, perfect for keeping all the outdoor stuff I would need to take care of a place like this in the woods. Perfect for taking off muddy boots and clothes. Perfect for hip waders and oars and for making birdhouses. And that tiny window over there – perfect as an exit into an outdoor aviary attached to a little dove cote I could build in here. It was, indeed, a perfect spot for us; a perfect house for Kev, and perfect gardens outdoors for me, with a garden room to boot. The whole place was just right for indoorsy Kevin and outdoorsy me.
We asked Carol, our agent, to contact the owner and see if we could buy it before it came on the market. We had only a couple of days, as purchasing beforehand isn’t allowed within two weeks of the planned offering date for the property. We barely had time. She took us back to our son’s house and dropped us off.
We walked into the house, thrilled to see the kids and our little granddaughter. Diana was looking unusually bright-eyed. We chatted a bit, and finally, she told me to read our one-year old granddaughter’s shirt. It said “Big sister.” I stared at it. “What,” I thought, “is going on?” There was no plan for another baby yet – the kids had to do in-vitro for that, and I knew they hadn’t started that arduous process again, not this soon after the first. “Is this a joke?” I asked. “No,” both Diana and Sam said. She held up an ultrasound image. “Is that an old ultrasound of Maeva? I asked. “No,” they both replied. “What?” I said. “How … what … is going on?” I was confused. Sam was wrought permanently sterile by chemotherapy a decade ago. Or so we all thought.
It turns out that sometimes men become fertile again a decade or so after a massive chemo regimen wipes out their fertility, and so it was with Sam. It was just an accident of fate. I cried, of course, because I cry about this sort of thing. Surprised, happy tears.
Then my phone rang. It was Carol. “The owner told me to go ahead and let you in the house to look and see if you really want it. She’d rather not go through the nightmare of listing and showing the house if you guys want it. I’ll pick you up in ten minutes.”
Once again, over the mountain and through the woods we went, in great anticipation, in shock from the kids’ news. We went in the house. Perfect size, perfect layout. Everything was wrong with it, though. Just a mess of foolishness. Mismatched window openers, crooked corners, improperly done trim, kooky doors; tv cables everywhere, including inside a closet, mismatched light bulbs, a stove that was broken, a dishwasher that was literally disintegrating, crooked drawer handles, mismatched light switches, and just tons of delayed and ignored maintenance. The basement had old, smelly, exposed insulation in the ceiling. Upon close inspection, the place was really, really dirty. It had been totally jury rigged. Nothing was quite right. There were trees growing in the gutters! And yet, we both knew it was the right place for us. We made an offer, and the seller took it, pending inspections, which proved to confirm that there were at least a hundred things that needed attention, but nothing structural.
The sellers knew they had us over a barrel. We really wanted the place. They insisted they get five months to move, an outrageous demand. They knew such an arrangement would leave us homeless for three months. Not their problem. They had no intention of making any repairs or doing any maintenance in the interim either. More things fell into disrepair while we waited. In the two months following possession, I lost fifteen pounds from the effort of attending to all of the things wrong with the place. Kev, who can’t afford to lose any weight, still lost ten. We ran back and forth to spend time with our granddaughter and relieve some of the pressure on the kids. Diana gave birth to little Ruby. It was a whirlwind of drama.
Now, already, the place is as we imagined it – magical, like a grandpa’s house should be. Everything is perfect. It’s organized, clean, properly painted, and pristine inside and out. The piano room looks lovely. The library is a place of comfort. The kitchen is perfect. The chipmunk nest has been removed from the dryer. Everything matches; everything is as squared up as it can be. Everything that was wrong has been fixed. The trees are trimmed. The gutters are covered. The gardens are cleaned up. Trees have been planted. Wildflowers have been sown. The forest edge has been softened. The pond has been cleaned, and the brook has been turned into a series of little pools and waterfalls. Next month I’ll be making a wood duck box in the garden room to put in one of the big pines by the pond. There’s a little dinghy on the pond now, the oars are hanging in the garden room with Maeva’s little life jacket which she’ll need in the spring when we row across the pond to have a picnic on the big rock by the spillway. Yesterday, I introduced her to the new doves in the garden room. She was exactly as thrilled as I hoped she’d be.

A review of the 2024 play at The Hartford Stage

On Saturday, December 7th, we attended this play at the Hartford Stage in downtown Hartford, CT. The play has run there since 1998, and this year the original director for the play in 1998 returned to direct it again, and it was not disappointing!
We are new to the area and did not really know what to expect. It was easy to get to the theater and there was easy access to adjacent parking. The entrance to the Hartford Stage is attractive and the lobby well maintained. We were greeted by scary actors in ghostly costumes who were in high spirits and who directed us to where we should go. In the theater we found a beautiful stage with lots of space, surrounded by comfortable seating extending around the entire stage except the back. Bathroom access and concessions were readily available and easy to find.
We realized when we took our seats about twenty minutes before the play started that there were significant numbers of neuro-divergent kids and adults there with their families. Once we realized this, we were concerned that we had taken seats that were really meant for other families. We had bought tickets way back in the summer and there had been no indication of any special shows. Our concerns, however, were quickly alleviated as we saw the auditorium filled to only about two-thirds capacity just before starting time – there was plenty of room.
It turned out that this particular episode of A Christmas Carol was a special one billed as “sensory-friendly,” a fact we did not know about until the opening announcements. “Sensory-friendly” means that the production has been modified so that individuals with neuro-divergence can enjoy the play without sensory overload. There is a “Quiet Room” designated just outside the theater door where anyone who is feeling too stimulated by visual display or sounds can go at any time during the performance or during the intermission. There are no restrictions on movement, so people can come and go as needed. There is no expectation that the audience will be completely quiet during the performance. There were also warning mechanisms in place to give a heads-up just before any loud sounds or bright special effects. Whether or not the sound and lighting was modified throughout the show as well, I don’t know, but it didn’t matter.
We can’t really say enough about the quality of the play as it opened before us. The set, the staging, the sound, the costumes, the special effects – all perfection, and a version of artistic expression we had never seen before for this much-loved Christmas play. And the actors! Their character interpretation was incredible, and not just the leads. The secondary and minor characters, including all the kids in the show, demonstrated superior acting chops. Allen Gillmore played Ebenezer Scrooge to incredible effect. Likewise for Noble Shropshire who played Mrs. Dilber, the housekeeper. Rebecka Jones played the Spirit of Christmas Past with utter perfection and John Andrew Morrison’s version of the Spirit of Christmas Present was incredibly effective, both hilarious and terrifying. Mr. Shropshire returned as the ghost of Jacob Marley, rising up through the floor from the pits of hell to frightening special effects, about which I really can’t say enough. The entire show was absolutely engaging, just perfectly done! We found the entire experience to be just thrilling.
I also want to say that the spirit of this play has certainly not lost its edge. In fact, at this particular time in the world, the play could not be more on point. It shouldn’t take a scary ghost and the threat of an untimely death or an eternity in hell to get us all to be nice, should it. It shouldn’t take a tragedy to remind us we have only one life to live, and that life should be filled with compassion and concern for others. Michael Wilson’s direction of this play, along with the incredible acting, really drove this point home, as did watching it in a neurodivergent crowd. It was a total immersion experience.
If you can get to the play, go. It is riveting. You will come away with love in your heart and a renewed energy to be a better person.
God bless us, every one!
David Coster
Disclaimer: This rumination is my own perspective based on the culmination of a lifetime of thinking about and studying in science, medicine, sociology, anthropology, psychology, and theology.
I have always been bothered by the question, “Do you believe in God?”
There is a presumption about that question that is troublesome. The presumption is that the person being questioned knows what the questioner means by the word “God” and agrees with the questioner’s definition of the word, God. The receiver of the question thus cannot simply answer the question “yes” or “no” as the questioner did not actually define what it is they are talking about. It’s a trap.
In America, the person asking that question is typically a Christian that is looking to show the superiority of their religious belief system’s definition or perception of what or who God is, along with wanting to demonstrate their own overall superiority for being so familiar with that God – for knowing the One God, for being in the inner circle of God. In order to wield the superiority of their position within the inner circle of God, they have faith that their definition of God is correct, is widely accepted, and irrefutable. I think this positioning of oneself as superior may also be true for people who have different faiths, particularly if their faith is predominant in the culture in which they live. It is extremely off-putting to be lectured to by a person who has such feelings of religious superiority that they think they actually know God as if God is a person they can speak for and who is their best friend. While you, if you think God is something other than they do, are simply wrong. It’s a point of pride for the questioner to be so right, so sure of themselves.
So, when someone asks me “Do you believe in God?” I respond with “Yes, but probably not the way you do.”
The one thing I think we can all agree on is that “God” is whatever the thing or event is that caused the existence of all things.
To define what we mean when we use the word “God,” we have to be able to define what it was that set off the creation of the entire universe. Whatever it was that caused the universe to exist, it is likely impossible to ever know or accurately define it. It seems logical to me that the universe itself, and everything in it, is “God,” from radiation and light waves to all elements and compounds and to all the material things that exist, including living things. It seems logically intuitive that everything that exists, visible or invisible, is made of “God” and is, therefore, “God.”
So, where then do we look for “God?” In that rock over there? That stream? That plant? That volcano? That sunlight? That star? The northern lights? The air? In magnetism? Electricity? Stars? Black holes? Animals? In us? Is “God” in everything? Is everything made of and by “God?” I think so. I think God is everywhere, and God is everything.
As humans, we are literally made up of all the components of the Periodic Table of the Elements, just like stars and comets and planets. We coexist with invisible things that can go right through us without us being aware – all sorts of miniscule particles and waves, all coming from the universe. Our bodies are a hive of living organisms – viruses, bacteria, fungi, parasites, and etc., living on us and in us. The levels of the particles within us, whether they be elements or microscopic forms of life, can determine whether or not we are alive and can exist as an organism. Too much or too little potassium, sodium, magnesium, chromium, iron, calcium, lead, zinc, oxygen, carbon, or chemical compounds like water and amino acids, and vitamins, and we cease to exist as a living identifiable entity; rather, we die and disintegrate, returning back to the basic elements of which we were made in the first place, the elements that make up everything in the universe. And those can be broken down further into protons and neutrons and electrons and even smaller particles. We are made of all those things, just like the rest of the universe.
I believe the mistake we have made is to try to make “God” manageable on a human scale by attributing “it” with male human characteristics. Yes, I said “it,” not he, not she, not them.” If God is the force and material that brought everything into existence, then God cannot be limited to the thing that many religions make it – a human-like invisible entity watching us and interfering with our daily lives. It is comical to note that the God for each culture and religion is exactly what the people of that religion want God to be. In each religion, the religious leaders are dictating to their converts what God is and what God wants them to do and be. In other words, God is being created and defined by Mankind, not the other way around.
If one replaces the term “God” in all religious texts with “the force” or “the universe” the text suddenly becomes clear and believable. Everything that happens on earth is a consequence of being part of the universe, a universe that functions in its own way and of its own accord, following rules of which only some we understand. The universe is in us, and we are in the universe. We are imbued with the universe; we are made of it. We are made of God. We therefore cannot be separated from God. God is in us and of us, and we are in God and of God. God is the universe; the universe is God.
I choose to believe that God is the universe and all the forces within it, and it gives me great peace to think I am made of God-particles that follow the rules of the universe rather than the rules of religious belief systems. When I say I feel at one with God, that’s because I am in God, and God is in me. We are the same thing. Just like that rock over there. Or that sun. Or that stellar dust cloud way out in the universe.
Do I have a soul? A ghost? That’s a super interesting question. I’ve had experiences that make me think there is something within us that still exists after our bodies disintegrate, something that is also a part of the universe, something that flies away “out there” when we take our last breath. If we have a soul and it’s part of the universe, why wouldn’t it just realign with the great beyond in some non-understandable way once we die? Why wouldn’t it continue to be part of God?
Could God be a force that is everywhere and in everything, but also a force that is aware of itself? Does the universe have a soul? Could all of the empty space actually be filled with the essence of a sentient force? I don’t know, but if a soul can exist, I don’t see why the universe couldn’t be sentient. If it is sentient, and we are part of it, then we are all just part of the greater organism, the universe.
I think it’s interesting that our DNA always remains alive and functioning within the entire human population, and much of it is shared with other species. In essence, life is an eternal web of DNA. The death of an individual organism is not the end of life as the individual’s DNA is living all over the place in others. Life never ceases. It just goes on and on. This is certainly a mysterious aspect of the universe. And even when Earth ceases to exist, life will still be in the universe, life that is related to life here. It’s all one and the same.
Several years ago, I was gardening out front on an early Sunday morning when a neighbor walked by and said, “You should be in church!” Without missing a beat I replied, “I am.” And I was. If “in church” means communing with God, then I’m “in church” wherever I am. If God is in me, I am always with God.
With the way I define “God,” I don’t need a religious belief system or a place of worship. I don’t need to listen to any other person’s spiel about their religious belief system – the concept of God does not require a religion to support it. The concept of God as everything supports itself, and the opinions of humans are neither here nor there – they have no impact on God’s existence. God does not need the confines of a religious framework in which to exist when God is everything, and God does not need human beings to make the rules about what God wants. The definition of God I use is one that can’t want anything – it just is.
If humans simply followed the golden rule – “Treat others as you would like to be treated,” – there would be no basis for the existence of any religious belief system. It would be a world without sin.
In a nutshell, I think that God is everything. I think ancient people knew this. They selected certain objects to deify in response to their feeling of wonder over the power of the universe, like the sun, or the wind, or the sea. It was a way to express their appreciation for an existence they couldn’t understand. I think that looking outward allows us to imagine the power of God, but for humans, because we are alive, the real place to look is inward. God is inside of us. The more I learn about the intricacies and expanse of the universe and the body, the clearer this concept becomes for me.
At this point in life, I tune out anyone who lectures me about what God wants or thinks. I tune out anyone who says I am going to some eternal hell of one sort or another if I don’t follow the same religious beliefs. I tune out anyone who says they have a personal relationship with a human-like invisible God-entity, one they must pray to if they wish to communicate with it – if one believes they are made of God, they have only to look inward or outward to find it and meld their mind with it.
I also tune out people who say that prayer works, unless they simply mean that saying a prayer makes them feel better. I’m sure it does – it feels like you’re doing something good even if you’re actually doing nothing tangible to help. God helps those who help themselves. And if we are a part of God, there’s no other way to make things better for others than to do it ourselves. That’s how God gets things done. I want to be clear: prayer does not help when someone needs food, shelter, moral support, a hug, advice, or anything else tangible. It is just another imagined position of religious superiority for the person saying the prayer, a person who is too lazy or too unkind to actually do something and make the concept of God actually work and do something constructive.
What if someone is praying for themself, though? It still seems preposterous to me, still a sort of pretention, but maybe sometimes it’s a way of meditating or looking inward. But even so, nothing will get better unless the person doing the praying gets off their butt and solves the problem at hand or asks for help from people who can solve it for them.
There are those who make claims that God is “telling” them – through their religion – to treat certain other types of people badly. Or that he needs them to mistreat others on His behalf. (I’ve always found it funny that this particular version of God is unable to act on His own behalf and harm the people he doesn’t like himself; he’s too weak, I guess, and has to rely on the wickedness of his worshippers to do His dirty work.) This is particularly egregious, whether it be the genocide being inflicted on the Palestinians by the Jews, the Muslim extremists in Afghanistan abusing women, or the Evangelicals terrorizing the trans community in America. This version of God, the one which is just a reflection of the vileness of those who created Him, should be thrown into the trash bin permanently.
God cannot be the light if God is full of hate and wields it through His worshippers. The God our religions have created therefore cannot be God at all. God is entirely something else than our main religious constructs claim He is. I like my definition of God much better. It makes no excuses for the bad behavior of mankind, forcing mankind to look in the mirror and take responsibility for its own actions, just like the Universe dictates we must. When everything ends for humans someday, the God of our big religious institutions will be nowhere to be found to help or change the outcome. Why? Because that God was never there in the first place.
